Predictive policing is a term that refers to proactive
police techniques that are based on software program projections, particularly
on high-risk areas and periods.
Since the late 2000s, these tactics have been progressively
used in the United States and in a number of other nations throughout the
globe.
Predictive policing has sparked heated debates about its
legality and effectiveness.
Deterrence work in policing has always depended on some type
of prediction.
Furthermore, from its inception in the late 1800s,
criminology has included the study of trends in criminal behavior and the
prediction of at-risk persons.
As early as the late 1920s, predictions were used in the
criminal justice system.
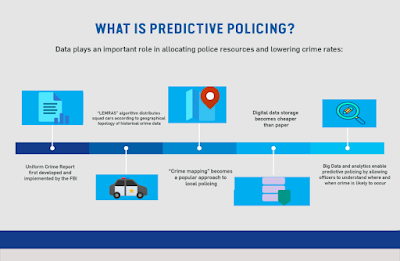
Since the 1970s, an increased focus on geographical
components of crime research, particularly spatial and environmental
characteristics (such as street lighting and weather), has helped to establish
crime mapping as a useful police tool.

Since the 1980s, proactive policing techniques have
progressively used "hot-spot policing," which focuses police
resources (particularly patrols) in regions where crime is most prevalent.
Predictive policing is sometimes misunderstood to mean that
it prevents crime before it happens, as in the science fiction film Minority
Report (2002).
Unlike conventional crime analysis approaches, they depend
on predictive modeling algorithms powered by software programs that
statistically analyze police data and/or apply machine-learning algorithms.

(1) locations and times when crime is more likely to occur;
(2) persons who are more likely to conduct crimes; and
(3) the names of offenders and victims of crimes.
"Predictive policing," on the other hand,
generally relates mainly to the first and second categories of predictions.
Two forms of modeling are available in predictive policing
software tools.
The geospatial ones show when and where crimes are likely to
occur (in which area or even block), and they lead to the mapping of crime
"hot spots." Individual-based modeling is the second form of
modeling.
Variables like age, criminal histories, gang involvement, or
the chance of a person being engaged in a criminal activity, particularly a
violent one, are used in programs that give this sort of modeling.
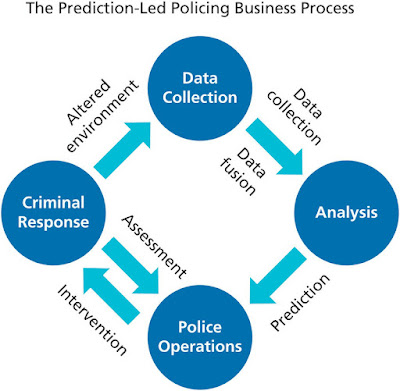
These forecasts are often made in conjunction with the
adoption of proactive police measures (Ridgeway 2013).
Police patrols and restrictions in crime "hot
areas" are naturally included in geospatial modeling.
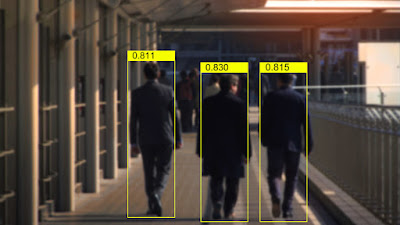
Individuals having a high risk of becoming involved in
criminal behavior are placed under observation or reported to the authorities
in the case of individual-based modeling.
Since the late 2000s, police agencies have been
progressively using software tools from technology businesses that assist them
create projections and implement predictive policing methods.
With the deployment of PredPol in 2011, the Santa Cruz
Police Department became the first in the United States to employ such a
strategy.

More than sixty police agencies throughout the United States
already employ PredPol.
In 2012, the New Orleans Police Department was one of the
first to employ Palantir to perform predictive policing.
Since then, many more software programs have been created,
including CrimeScan, which analyzes seasonal and weekday trends in addition to
crime statistics, and Hunchlab, which employs machine learning techniques and
adds weather patterns.
Some police agencies utilize software tools that enable
individual-based modeling in addition to geographic modeling.
The Chicago Police Department, for example, has relied on
the Strategic Subject List (SSL) since 2013, which is generated by an algorithm
that assesses the likelihood of persons being engaged in a shooting as either
perpetrators or victims.
Individuals with the highest risk ratings are referred to
the police for preventative action.
Predictive policing has been used in countries other than
the United States.
PredPol was originally used in the United Kingdom in the
early 2010s, and the Crime Anticipation System, which was first utilized in
Amsterdam, was made accessible to all Dutch police departments in May 2017.
Several concerns have been raised about the accuracy of
predictions produced by software algorithms employed in predictive policing.
Some argue that software systems are more objective than
human crime data analyzers and can anticipate where crime will occur more
accurately.
Predictive policing, from this viewpoint, may lead to a more
efficient allocation of police resources (particularly police patrols) and is
cost-effective, especially when software is used instead of paying human crime
data analysts.
On the contrary, opponents argue that software program
forecasts embed systemic biases since they depend on police data that is itself
heavily skewed due to two sorts of faults.
To begin with, crime records appropriately represent law
enforcement efforts rather than criminal activity.
Arrests for marijuana possession, for example, provide
information on the communities and people targeted by police in their anti-drug
efforts.
Second, not all victims report crimes to the police, and not
all crimes are documented in the same way.
Sexual crimes, child abuse, and domestic violence, for example, are generally underreported, and U.S. citizens are more likely than non-U.S. citizens to report a crime.
For all of these reasons, some argue that predictions
produced by predictive police software algorithms may merely tend to repeat
prior policing behaviors, resulting in a feedback loop: In areas where the
programs foresee greater criminal activity, policing may be more active,
resulting in more arrests.
To put it another way, predictive police software tools may
be better at predicting future policing than future criminal activity.
Furthermore, others argue that predictive police forecasts
are racially prejudiced, given how historical policing has been far from
colorblind.
Furthermore, since race and location of residency in the
United States are intimately linked, the use of predictive policing may
increase racial prejudices against nonwhite communities.
However, evaluating the effectiveness of predictive policing
is difficult since it creates a number of methodological difficulties.
In fact, there is no statistical proof that it has a more
beneficial impact on public safety than previous or other police approaches.
Finally, others argue that predictive policing is
unsuccessful at decreasing crime since police patrols just dispense with
criminal activity.
Predictive policing has sparked several debates.
The constitutionality of predictive policy's implicit
preemptive action, for example, has been questioned since the hot-spot policing
that commonly comes with it may include stop-and-frisks or unjustified
stopping, searching, and questioning of persons.
Predictive policing raises ethical concerns about how it may
infringe on civil freedoms, particularly the legal notion of presumption of
innocence.
In reality, those on lists like the SSL should be allowed to
protest their inclusion.
Furthermore, police agencies' lack of openness about how
they use their data has been attacked, as has software firms' lack of
transparency surrounding their algorithms and predictive models.
Because of this lack of openness, individuals are oblivious
to why they are on lists like the SSL or why their area is often monitored.
Members of civil rights groups are becoming more concerned
about the use of predictive policing technologies.
Predictive Policing Today: A Shared Statement of Civil
Rights Concerns was published in 2016 by a coalition of seventeen
organizations, highlighting the technology's racial biases, lack of
transparency, and other serious flaws that lead to injustice, particularly for
people of color and nonwhite neighborhoods.
In June 2017, four journalists sued the Chicago Police
Department under the Freedom of Details Act, demanding that the department
provide all information on the algorithm used to create the SSL.
While police departments are increasingly implementing
software programs that predict crime, their use may decline in the future due
to their mixed results in terms of public safety.
Two police agencies in the United Kingdom (Kent) and
Louisiana (New Orleans) have terminated their contracts with predictive
policing software businesses in 2018.
Find Jai on Twitter | LinkedIn | Instagram
You may also want to read more about Artificial Intelligence here.
See also:
Clinical Decision Support Systems; Computer-Assisted Diagnosis.
References & Further Reading:
Collins, Francis S., and Harold Varmus. 2015. “A New Initiative on Precision Medicine.” New England Journal of Medicine 372, no. 2 (February 26): 793–95.
Haskins, Julia. 2018. “Wanted: 1 Million People to Help Transform Precision Medicine: All of Us Program Open for Enrollment.” Nation’s Health 48, no. 5 (July 2018): 1–16.
Madara, James L. 2016 “AMA Statement on Precision Medicine Initiative.” February 25, 2016. Chicago, IL: American Medical Association.
Morrison, S. M. 2019. “Precision Medicine.” Lister Hill National Center for Biomedical Communications. U.S. National Library of Medicine. Bethesda, MD: National Institutes of Health, Department of Health and Human Services.