
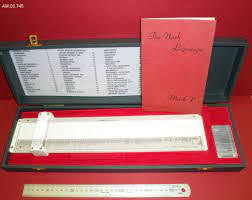
Firmin Nash, director of the South West London Mass X-Ray Service, devised the Group Symbol Associator, a slide rule-like device that enabled a clinician to correlate a patient's symptoms against 337 predefined symptom-disease complexes and establish a diagnosis in the early 1950s.
It resolves cognitive processes in automated medical
decision-making by using multi-key look-up from inverted files.
The Group Symbol Associator has been dubbed a
"cardboard brain" by Derek Robinson, a professor at the Ontario
College of Art & Design's Integrated Media Program.
Hugo De Santo Caro, a Dominican monk who finished his index
in 1247, used an inverted scriptural concordance similar to this one.
Marsden Blois, an artificial intelligence in medicine
professor at the University of California, San Francisco, rebuilt the Nash
device in software in the 1980s.
Blois' diagnostic aid RECONSIDER, which is based on the
Group Symbol Associator, performed as good as or better than other expert
systems, according to his own testing.
Nash dubbed the Group Symbol Associator the
"Logoscope" because it employed propositional calculus to analyze
different combinations of medical symptoms.
The Group Symbol Associator is one of the early efforts to
apply digital computers to diagnostic issues, in this instance by adapting an
analog instrument.
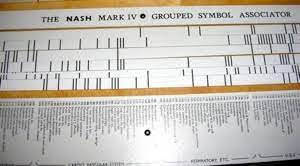
Along the margin of Nash's cardboard rule, disease groupings
chosen from mainstream textbooks on differential diagnosis are noted.
Each patient symptom or property has its own cardboard
symptom stick with lines opposing the locations of illnesses that share that
property.
There were a total of 82 sign and symptom sticks in the
Group Symbol Associator.
Sticks that correspond to the state of the patient are
chosen and entered into the rule.

Nash's slide rule is simply a matrix with illnesses as
columns and properties as rows.
Wherever qualities are predicted in each illness, a mark
(such as a "X") is inserted into the matrix.
Rows that describe symptoms that the patient does not have
are removed.
The most probable or "best match" diagnosis is
shown by columns with a mark in every cell.
When seen as a matrix, the Nash device reconstructs
information in the same manner as peek-a-boo card retrieval systems did in the
1940s to manage knowledge stores.
The Group Symbol Associator is similar to Leo J. Brannick's analog computer for medical diagnosis, Martin Lipkin and James Hardy's McBee punch card system for diagnosing hematological diseases, Keeve Brodman's Cornell Medical Index Health Questionnaire, Vladimir K.
Zworykin's symptom spectra analog computer, and other
"peek-a-boo" card systems and devices.
The challenge that these devices are trying to solve is
locating or mapping illnesses that are suited for the patient's mix of
standardized features or attributes (signs, symptoms, laboratory findings,
etc.).
Nash claimed to have condensed a physician's memory of
hundreds of pages of typical diagnostic tables to a little machine around a
yard long.
Nash claimed that his Group Symbol Associator obeyed the
"rule of mechanical experience conservation," which he coined.
"Will man crumble under the weight of the wealth of
experience he has to bear and pass on to the next generation if our books and
brains are reaching relative inadequacy?" he wrote.
I don't believe so.
Power equipment and labor-saving gadgets took on the
physical strain.
Now is the time to usher in the age of thought-saving
technologies" (Nash 1960b, 240).
Nash's equipment did more than just help him remember
things.
He asserted that the machine was involved in the diagnostic
procedure' logical analysis.
"Not only does the Group Symbol Associator represent
the final results of various diagnostic classificatory thoughts, but it also
displays the skeleton of the whole process as a simultaneous panorama of
spectral patterns that correlate with changing degrees of completeness,"
Nash said.
"For each diagnostic occasion, it creates a map or
pattern of the issue and functions as a physical jig to guide the mental
process" (Paycha 1959, 661).
On October 14, 1953, a patent application for the invention
was filed with the Patent Office in London.
At the 1958 Mechanization of Thought Processes Conference at
the National Physical Laboratory (NPL) in the Teddington region of London, Nash
conducted the first public demonstration of the Group Symbol Associator.
The NPL meeting in 1958 is notable for being just the second
to be held on the topic of artificial intelligence.
In the late 1950s, the Mark III Model of the Group Symbol
Associator became commercially available.
Nash hoped that when doctors were away from their offices
and books, they would bring Mark III with them.
"The GSA is tiny, affordable to create, ship, and
disseminate," Nash noted.
It is simple to use and does not need any maintenance.
Even in outposts, ships, and other places, a person might
have one" (Nash 1960b, 241).
Nash also published instances of xerography (dry
photocopying)-based "logoscopic photograms" that obtained the same
outcomes as his hardware device.
Medical Data Systems of Nottingham, England, produced the
Group Symbol Associator in large quantities.
Yamanouchi Pharmaceutical Company distributed the majority
of the Mark V devices in Japan.
In 1959, Nash's main opponent, François Paycha, a French
ophthalmologist, explained the practical limits of Nash's Group Symbol
Associator.
He pointed out that in the identification of corneal
diseases, where there are roughly 1,000 differentiable disorders and 2,000
separate indications and symptoms, such a gadget would become highly
cumbersome.
The instrument was examined in 1975 by R. W. Pain of the
Royal Adelaide Hospital in South Australia, who found it to be accurate in just
a quarter of instances.
You may also want to read more about Artificial Intelligence here.
See also:
Computer-Assisted Diagnosis.
Further Reading:
Eden, Murray. 1960. “Recapitulation of Conference.” IRE Transactions on Medical Electronics ME-7, no. 4 (October): 232–38.
Nash, F. A. 1954. “Differential Diagnosis: An Apparatus to Assist the Logical Faculties.” Lancet 1, no. 6817 (April 24): 874–75.
Nash, F. A. 1960a. “Diagnostic Reasoning and the Logoscope.” Lancet 2, no. 7166 (December 31): 1442–46.
Nash, F. A. 1960b. “The Mechanical Conservation of Experience, Especially in Medicine.” IRE Transactions on Medical Electronics ME-7, no. 4 (October): 240–43.
Pain, R. W. 1975. “Limitations of the Nash Logoscope or Diagnostic Slide Rule.” Medical Journal of Australia 2, no. 18: 714–15.
Paycha, François. 1959. “Medical Diagnosis and Cybernetics.” In Mechanisation of Thought Processes, vol. 2, 635–67. London: Her Majesty’s Stationery Office


